Psychoactive Drugs Handout
Doc … can I get a copy of your slides?
That is one of the most common requests I field after presentations. I totally understand, as there is a lot of information there, and it can be somewhat overwhelming. However, just printing out or copying the slides winds up killing a lot of trees and does not necessarily convey all of the information in the presentation! Here, then, is all the information presented in the slides, along with some necessary explanations.
The major three points of the talk are:
-
All psychoactive drugs impair, they just do it differently, and over different time courses. We are not usually aware of what such different impairment looks like – we’re only familiar with alcohol.
-
A drug is a drug, there is no such thing as soft or hard drugs – just different. Alcohol is a drug.
- People who are impaired, particularly long-term impairment, are usually unaware of this.
All psychoactive drugs have effects both on your brain, and on your body. They include the acute period when the drug is actively working on your brain, the so-called intoxication phase, and the aftereffects of the drug as your body is slowly metabolizing or eliminating it, the so-called “hangover phase”. Depending on the drug, some of these late, post intoxication effects, can last for several weeks after your last use if you are a heavy or regular user.
In our society we are fond of classifying drugs as “soft” or harmless, versus “hard” or dangerous. This is at best foolish, and at worst deadly. There are no such things as soft or hard drugs. A drug is a drug. Some of them have more dangerous side effects, some of them have more addiction potential for certain individuals than others, but these are relatively minor points. If you are addicted to marijuana, or you are killed because of its late effects on concentration or coordination, it is scarcely a “soft drug”. Some people take cocaine and don’t become addicted. Does that make it a “soft” drug?
There are two very different groups of people in society, and educators often do not explain which group they are discussing when they are talking about psychoactive drugs. The first group, comprising about 90% of people, are not addicted. They may be impaired, and they may be killed or injured as a result of their impairment, but they can still make choices about when, where, and how much they use. The remaining 10% have lost those choices and have become addicted to their drug, or drugs of choice. They tend to suffer more long-term harm in terms of brain damage and body damage, and they tend to be impaired for longer periods of time. They are usually unaware that they have a problem. There is only one response to addiction and that is to stop using all psychoactive substances permanently. At the end of these notes I reprint the explanation of addiction, recovery, and freedom of choice as written by Cpt. Lyle Prouse, one of the NorthWest Airlines pilots jailed for flying under the influence of alcohol. It is one of the best explanations of addiction “from inside the belly of the beast” that I have ever read.
The following are some of the facts and figures which interest most audiences and appeared in the slides:
- Worker absenteeism attributed to substance abuse costs Alberta economy approx. $720 million/year (1996).
- More than 12,000 Alberta Workers yearly know of a workplace injury(ies) that they believe were related to drug or alcohol use.
- Direct losses in the Canadian workplace in 1992 were $4.2 billion.
- In Alberta, 1995, 20.4% of all drivers in fatal crashes had been drinking.
- Alcohol Basic facts:
- Sedative/hypnotic
- Rapidly absorbed, slowed by food, water soluble
- Eliminated by first order kinetics, (slower in women), 10 gm/hr
- Converted to acetaldehyde then to acetate
- One drink in North America = 13.6 grams EtOH
- Amount of pure ethanol calculated by %abv x .78 = gm EtOH/100 ml
Canadian Data:
- National average 79.3% drank in past year; 1994 = 72.3%
- 2/3 are light drinkers
- 10% heavy frequent drinkers
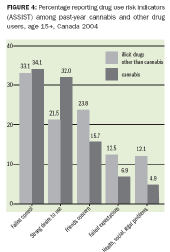
Harms
- Passenger with drunk driver - 7.5% in 1994; 17.8% in 2004!
- Physical health harmed – 12% 1994; 15% 2004
CADUMS 2011 – Canadian Alcohol and Drug Use Monitoring Survey
- Statistically significant increases in heavy infrequent drinking among males and adults and light frequent drinking in females
- 78% adults drank in last year
- 14.4% exceed low risk guidelines
- 14.6% report at least one harm (down from 28.3%), but last year harm remained the same
Wine:
- One 750 ml bottle of wine contains 76 gm EtOH (13%) or 82 gm (14%), 5.6 or 6.03 standard drinks
- A litre of wine contains 7.5 or 8.03 drinks
- Sparkling wines are typically 10-11% abv
- Wine glasses typically range from 4-12 oz (114-342 ml) i.e. a bit less than 1-3 standard drinks
- Sherry is 20% abv, Dubonnet = 16%; 1 standard drink is 87 ml (2 shot glasses) and 109 ml respectively
Beer:
- Standard beer is 5% abv, 355 ml bottles which is 13.8 gm/bottle; 1.0 standard drinks.
- Strong beer = (6-11%) 9.0% abv; 24.92 gm/bottle; 1.8 standard drinks
- Lite beer = 4% = 11 gm/bottle = .8 standard drinks
- Supercans = 473 ml; 1 supercan of Wildcat = 22.3 gm, 1.7 standard drinks
- Also available in 650 and 950 ml cans
- 1 pint = 2 cups = 455ml = 17 gm EtOH = 1.25 drinks; 2 pints = 2.5 standard drinks
- Pitcher = approx 1.5 litre = 58 gm = 4.25 drinks
- “Boilermaker” is 1.5 oz Vodka added to beer; 17 gm + 13.4 gm = 30 gm = 2.25 drinks
Spirits:
- Proof is 2x abv. Most spirits are 40% abv
- One standard drink is 44 ml, 1.5 oz
- Shot glass holds approx 50 ml, 1.2 drinks
- 750 ml bottle holds 234 gm, 17.2 drinks; 1.14 l bottle holds 355 gm, 26.1 drinks
- Liqueurs range from 16% (Bailey’s) to 40% (most)
- Studies show most people err by 2.5 to 3 times in optical volume measurements
Blood Alcohol Concentration (BAC):
- BAC – Blood Alcohol Concentrations. Measured in grams/100 ml blood.
- .01 – marked increase in sleepiness. Impairs sleep.
- .02 – decreased ability to understand commands, esp. radio.
- .03 risk of fatal MVA 1.5x normal
- .05 – too impaired to operate a vehicle. 24 hour suspension. Poor speed/distance perception. Poor problem solving skills. Fatal MVA 2 x normal.
- .08 – “legally” impaired. Fatal MVA 4 x normal.
- .1-.19 – neurologic impairment, reaction time, ataxia..
- .2-.3 – severe impairment
- .4 – hypothermia, stage 1 anaesthesia, aspiration
- .5-.8 – onset of coma, death
Time course of intoxication:
- Metabolism decreases BAC by .015 per hour
- Average male reaches .08 after 3-4 standard (2-3 for women) drinks in one hour
- A typical “night out” sees a BAC of .1 to .2 (10 -20 standard drinks)
- Return to BAC of 0 will take more than 10 hours after last drink.
-
Impairment will last 20 – 30 hours
- 1 a.m. Drives home drunk BAC.165
- 2 a.m. Worker goes to bed .15
- 3 a.m. Sleeping .135
- 4 a.m. Bathroom .120
- 5 a.m. Restless .105
- 7 a.m. Alarm goes off .075
- 8 a.m. Drives to work impaired .060
- 8:30 a.m. Begins work impaired .055
- Noon 0.0
- Afternoon – hung over impairment continues
Marijuana
- Most recent nation-wide survey published is 2004
- Marijuana usage increased over 1994 from 7% - 14% population
- Males 18.2% ; females 10.2%
- 70% of those 18-24 yrs used lifetime
- 30% 15-17 ; 47% 18-19 used in past yr.
- Lifetime use 44%
- 34.9% no high school; 52.4% college; 44.2% univ
- Among current users 20.3% use weekly; 18.1% use daily
CADUMS 2011
- Past year use down from 14% to 9.1%
- Males 12.2% (vs 18) and Females 6.2% (vs. 10.2)
- Youth still 2-3x usage of adults.
- Past year use – youth = 21.6%
- Average age of initiation 15.6 years
“Medical” Marijuana
- Note: The College of Physicians & Surgeons of Alberta recommends that physicians do not prescribe marijuana to patients. This recommendation is based on the lack of scientific evidence regarding medical marijuana’s risks and benefits and the lack of clarity surrounding civil litigation risks.
If you decide to prescribe marijuana, you need to ensure your complete compliance with the complex regulations outlined by Health Canada.
- Complex mixture of > 400 chemicals; 66 are cannabinoids; active ingredient is delta 9 tetrahydrocannabinol
- MJ in 60’s typically 3-5%, now typically 10%, can be 40% (hash oil, BC bud)
- Fat soluble (vs. EtOH)
- Long ½ life
- Binds to brain receptors, esp cerebellum (driving) and hippocampus (learning); cumulative drug load
- Extreme tolerance develops quickly
Physical:
- Some estimates 20x carcinogenicity of cigarettes; (and additive to) – 50-70% more carcinogenic hydrocarbons
- CAD, cardioacceleration, MI risk 4x in first hour
- Anti-androgen, anti-estrogen
- THC crosses placental barrier, milk
- “Mom’s marijuana use alters baby’s brain function” Medical Post May 6, 2003; Ottawa Prenatal Prospective Study, fMRI, 35 kids followed since 1978
Psychological
- Perceptual distortion, esp time/distance, peripheral vision, colour, attention.
- Learning impaired – lasts 4 weeks? (Pope 2001)
- Addiction liability – similar to opiate w/d, less than coc.
- Classic W/D syndrome, esp. aggression, peaks @ 1 wk. U of Vermont study 6.3/9 criteria DSM IV
- Took 3 weeks post w/d for daily users to drop to control levels
“Dose related neurocognitive effects of marijuana use” Bolla et al. Neurology 2002;59:1337-1343
“As joints smoked per week increased, performance decreased on tests measuring memory, executive functioning, psychomotor speed and manual dexterity”
Cognitive impairment measurable at 1 week abstinence, disappears by 4 weeks. Dr. Harrison Pope, NIDA
“Cerebrovascular perfusion in marijuana users during a month of monitored abstinence” Herning et al. Neurology 2005;64:488-493
“Chronic marijuana use is associated with increased cerebrovascular resistance through changes mediated in blood vessels or brain parenchyma. These findings may provide a partial explanation for the cognitive deficits observed in a similar group of marijuana users.”
THC Impairment
- Much worse in adolescent brain
- Greatest long lasting effects on
- impulsivity
- risk taking
- and decision making (4 weeks)
- Paradoxical effect on attention/concentration in heavy users
-
Increasing amounts of research on working memory, recall
- The marijuana – schizophrenia link
- Swedish study – 50,000 men followed for 27 years
- 50 x by age 18 increased schizophrenia by 30%
- 13% of all cases could be prevented by eliminating marijuana
- British study – 1/10 smokers dx schiz by age 26
- The depression link
- 6 year study of 2000 adolescent girls in NZ
- Daily users 5x likely to become depressed
- Gateway drug – myth or fact?
- 63.4% of lifetime users report only cannabis
- 79.1% of past year users same
Does Marijuana increase car accident risk?
- Smoking pot doubles car accident risk
- Canadian Study, Dr. Mark Asbridge, Dalhousie, February 2012
- Pot < 3 hours before driving
- Meta analysis of 49,411 drivers
- Strongest link with fatal accidents
- 2004 – 4% of Canadians reported driving less than 1 hour after smoking. 1996 – 1.9%
Does Marijuana cause lung cancer?
- Yes (but not COPD)
- Earlier studies showed no effect due to poor controls, low numbers and flawed methodology
- Cannabis use and risk of lung cancer: a case-control study. Aldington et al
- Eur Respir J. 2008 Feb;31(2):280-6.
- The risk of lung cancer increased 8% (95% confidence interval (CI) for each joint-yr of cannabis smoking, after adjustment for confounding variables including cigarette smoking,
- and 7% (95% CI 5-9) for each pack-yr of cigarette smoking, after adjustment for confounding variables including cannabis smoking.
- The highest tertile of cannabis use was associated with an increased risk of lung cancer (relative risk 5.7 , after adjustment for confounding variables including cigarette smoking.
- In conclusion, the results of the present study indicate that long-term cannabis use increases the risk of lung cancer in young adults.
Other drugs, CADUMS 2011: Past year use:
- Ecstasy - .7%
- Cocaine - .9%
- Amphetamines - .5%
- 1 of 6 drugs including THC = 9.4% (vs. 14.5% in 2004)
- Any drug – 9.9% (23% age 15-24)
Cocaine
- Faster route – more intense effects
- Initial impairment through euphoria/ poor judgment – to paranoia – to acute psychosis
- Secondary impairment through “crash” and craving
- Tertiary impairment through brain chemistry alteration and rapid development of addiction
- Massive cardiac and respiratory side effects esp malignant arrythmia (risk 24x normal in first hour after use)
- Seizures, (sensitization), sudden death
Crystal Meth
- Man made analog of amphetamine. Smokable. Made in basement labs.
- Triggers massive release of dopamine – intense “rush”
- Neurotoxic in animal models – destroys dopamine and serotonin neurons (next slides). Long term damage
- Predisposition to neurodegenerative diseases later in life?
Ecstasy
MDMA – “E”
- Methylenedioxyamphetamine
- Hallucinogen, (euphoria, depression)
- Effects last 4-6 hours, after effects last weeks to months
- Works on serotonin system (mood)
- May damage neurons permanently after 1 use? (next slide)
- Addictive potential like very weak cocaine
- Malignant hyperthermia, chronic paranoid psychosis, cardiac arrest, coagulopathy
Latest evidence on Ecstasy
- Demonstrated cognitive decline after ecstasy use began. De Win et al, Arch Gen Psychiatry 2007; 64:728
- An imaging study finds evidence of brain damage in new users, compared with their own pre-use baseline and with ecstasy-naive controls. same authors, Brain 2008 Nov 131:2936
- The results are clear, Dr. de Win said, even short-term use of low doses of MDMA has long-term effects on the brain. She noted the change in perfusion was surprising. “From a pharmaceutical point of view, one would think the effects on blood flow would only last for a day or so, not the roughly four months seen here.”
Latest Trends
Alcohol and High Caffeine Drinks
- (4,275 college students from 10 universities)
- 24% mixed with alcohol in last 30 days
- Those mixing were more likely to ride with drunk driver 38.9% v 22.5 %
- Got injured more often 12.3% v 5.9%
- More likely to be sexually assaulted 6.4% v 3.7%
“Spice” – synthetic cannabinoids (marijuana)
- “Cyclone and all of the Organic Herbal Blends and ethnobotanicals available from this site are sold for collection, scientific research, education and propagation purposes only and that these products are not intended for human consumption. All customer should understand that all products offered on this site are void where prohibited, and that it is customers own responsibility to check and abide by local laws and regulations. Customers must be 19 or older purchase all ethnobotanicals from this site. By placing an order, you are agreeing to the disclaimer.”
“Bath Salts”
- mephedrone, pyrovalerone and methylenedioxypyrovalerone.
- Same/similar substances?
- Paranoia, interpersonal violence
- Crazy Train Bath Salt Fizz Concentrated Bath Salts Bolivian Bath salts Ivory Wave Bath salts Recharge Bath Salts eight ballz bath salt Loco Motion Bath Salts Revitalize Bath Salts Rave On Bath Salt Raving Dragon Bath Salts White Girl Concentrated Bath Salts Tranquility Concentrated Bath Salts Lady Bubbles Bath Salts X Rated Bath Salts Ivory Smooth Concentrated Bath Salts Blue Wave Bath Salts Bubbling 24 Bath Salts Blue Silk - Bath Salt G Pheonix Bath Salts Bliss Concentrated Bath Salts White Rush Bath Salts Blue Magic - Bath Salts
Summary
- Alcohol is alcohol. Alcohol is a drug
- A drug is a drug is a drug
- There are no “safe” or “soft” drugs. Just different.
- Impairment is quite different than intoxication
- All psychoactive drugs impair an person’s ability to work/learn safely – sometimes for several weeks after ingestion. Sometimes permanently.
- Almost everyone is unaware of the extent of their impairment
- There are no easy answers to drug use in society – even though everyone wants them!
Appendix: Lyle’s Story:
My name is Lyle Prouse and I was the infamous Northwest Airlines Captain back in March of ‘90 who was arrested on Northwest Flight 650 (FAR-MSP) for flying drunk, along with the copilot and second officer.
Subsequently, I was fired by NWA, stripped of my flight certificates, and lost my medical due to alcoholism. I became a national pariah, was sent to federal prison for 16 months, served 14, and went broke within 30 days of the arrest. Furthermore, the trial judge put sanctions on me to insure I’d never fly again due to my age (51 at the time).
I want to be clear about a number of things. First, I make no excuses, I accept complete responsibility, and I openly acknowledge that everything that happened to me was fair and appropriate. Period.
Having said that, let me turn to some of the comments offered by a number of pilots in this forum. Some of those comments indicate some knowledge and understanding of the subject of alcohol/alcoholism and some indicate ignorance bolstered by arrogance.
When I talk about alcoholism I separate the issues between the acts and behavior (and the consequences that flow from that) - and the disease itself.
Being an alcoholic does not relieve me of responsibility for what I do nor does it grant me any immunity or excuse anything. Anytime I commit an unlawful act, alcoholic or not, it’s incumbent upon me to accept the consequences of that act.
It should be noted that while alcoholism is not an excuse for behavior it very clearly explains a lot of it in the case of the alcoholic. It might surprise some to know that since I got sober over 16 yrs ago I’ve never flown drunk or received a DUI… Nor have I done any of the shameful, disgraceful, offensive, and embarrassing things that drunks routinely do.
One of THE first steps of recovery demands acceptance of personal responsibility and being accountable. So the talking heads, Bill O’Reilly for one, who declare that the only reason for treating alcoholism as a disease is so those with it can escape responsibility, is absurd beyond words. Those ideas only come from non-alcoholics…in my experience.
I have been sober since the date of my arrest, over 16 years and some nine months now. I am active in recovery, speak all over the United States and Canada (for free, of course), have been involved with virtually every major airline in their alcohol programs. I am of Native American heritage and I’ve spoken on reservations in the US and Canada, and at Native American sobriety conventions.
I served out my prison time, came out broke and disgraced, and eventually earned back each of the four licenses I needed, commencing with the private and doing it, quite literally, from the ground up…after the judge miraculously lifted the sanctions on me. I did it the same way I stay sober, one day at a time, one thing at a time, one step at a time, and one license at a time.
I’d never had a private license - I came out of the Marine Corps as a Vietnam vet and quickly acquired a Com’l ticket and inst rating after a quickie test…and was hired 3 weeks later by NWA (Aug ‘68). I had gone in as a barely 18 yr old private and I left 11 1/2 yrs later as a Captain and jet pilot with an excellent reputation.
Not quite four years after my arrest and imprisonment, the Pres/CEO of NWA, Mr. John Dasburg, personally reinstated me to full flight status at NWA. It was an act of personal courage on his part that the word “extraordinary” doesn’t even begin to approach.
I retired honorably at age 60, in Sept ‘98, as a 747 captain, having done all I could to fully vindicate all those who had believed in me. Additionally, the tough Minnesota judge who tried and sent me to prison suggested, as I retired, that I apply for a presidential pardon and said he’d support it even tho he’d NEVER supported a petition for pardon in his 16 yrs on the bench. Two years later I rec’d a Pres Pardon - a HUGE, life altering event for a federal felon!
To one contributor who said alcoholism is a lifetime disease and implied we who are recovering are delicately balanced on the razor’s edge and might relapse anytime, I say he is only partially correct. It is a lifetime disease, that’s why it’s called Alcohol-ISM and not Alcohol-WASM. But so is diabetes and a number of other chronic diseases. And, yes, some never make it, never recover, and never stay sober - and they die (both my parents took this disease to their graves).
But to discount the millions of us around the world who live good, productive, solid lives in recovery displays a shallow and ignorant way of thinking. And to say no alcoholic should ever be trusted in the cockpit because they might relapse is absurd. Anyone in the cockpit might keel over, have a stroke, heart attack, brain anueryism, or some other possible problem and it’s nonsense thinking to make a blanket pronouncement and condemnation of everyone based on what “might” happen.
Many don’t make it. But many don’t survive cancer, heart disease, and other calamities of life. The airlines have THE most successful rate of alcoholism recovery among any group, virtually double the norm in the rest of our society. And they do a good job of weeding out those who will not or cannot get sober - and that’s as it should be.
I’m well aware that there are those, still today, who think I should have been put against a wall and shot; and that I most certainly NEVER should have been allowed to fly again. Fortunately, I don’t think that reflects most of the heart and soul of the American character who, traditionally, support and encourage the underdog and applaud comebacks.
Alcoholism is a treatable, recoverable disease. Today there are over 3500 recovering alcoholic pilots flying for airlines. One of the leading docs I know (who’s worked in the aviation/alcoholism field for over 30 yrs) says, “When I get on the plane I glance in the cockpit. If it’s a face I recognize, I breathe a sigh of relief. If it’s one I don’t…then I sit in the back and wonder.”
To each his/her own. I doubt anything I’ve said here will change any minds and may only provoke further debate. My only purpose here is to speak the truth as I know it and do it quietly and clearly.
Being an alcoholic was something I first viewed as a disgraceful, shameful, stigmatic curse. It has evolved into the greatest thing that ever occurred to me because of what it has forced me to do. My kids won’t have to watch me die a grim, lingering alcoholic death, as I had to with my parents. My life today is geared toward giving back more than I ever took, making amends where ever possible, and being constantly grateful for the joy of sobriety and the brightness of each day.
What I have expressed here today is not something unique to me. It is shared by virtually every recovering person I know. I just came home a few minutes ago from speaking in Denver last night. As is always the case, I met people who inspire me and make me glad I was forced into a program of recovery I NEVER would have willingly accepted when I was drinking.
Blue skies, Lyle Prouse Ex federal inmate 04478-041 Ret’d NWA Capt 086140 Marine Capt 086099